
Local organisation turns to innovation to provide answers to donor fatigue for family planning
When contraceptives disappeared from Kilifi health facilities, Leila Abdulkheir turned a service gap into a governance issue. Using community data, digital tools and public participation forums, she pushed county officials to confront procurement failures, showing how local innovation can move beyond outreach to influence budgets, systems and accountability in reproductive health.
In Kilifi County, Health Care Providers often reply: “We do not know, disbursements have not arrived.”
When contraceptives disappear from health facilities, the consequences are immediate and measurable. Kilifi records the highest rate of teenage pregnancy in Kenya at 71%, with cases rising by 28.9%.
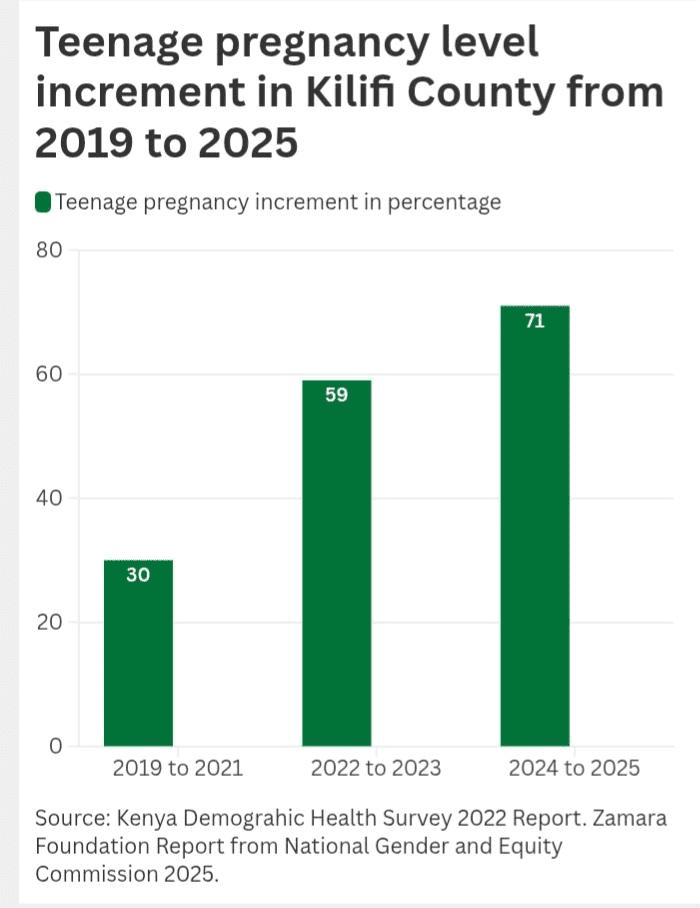
At the same time, Kilifi County Government funding for family planning has declined from 26% to 16% in recent years.
These shortages reflect a broader systemic breakdown. Nationally, 6.6 million women of reproductive age rely on modern contraceptives, with 62% accessing them through public health facilities. Stock-outs in counties like Kilifi are therefore not isolated failures; they disrupt the primary source of care for millions.
Leila Abdulkheir moved quickly. She mobilised digital tools, trained community health volunteers, ran trauma-informed adolescent circles, and carried community demands into county policy rooms.
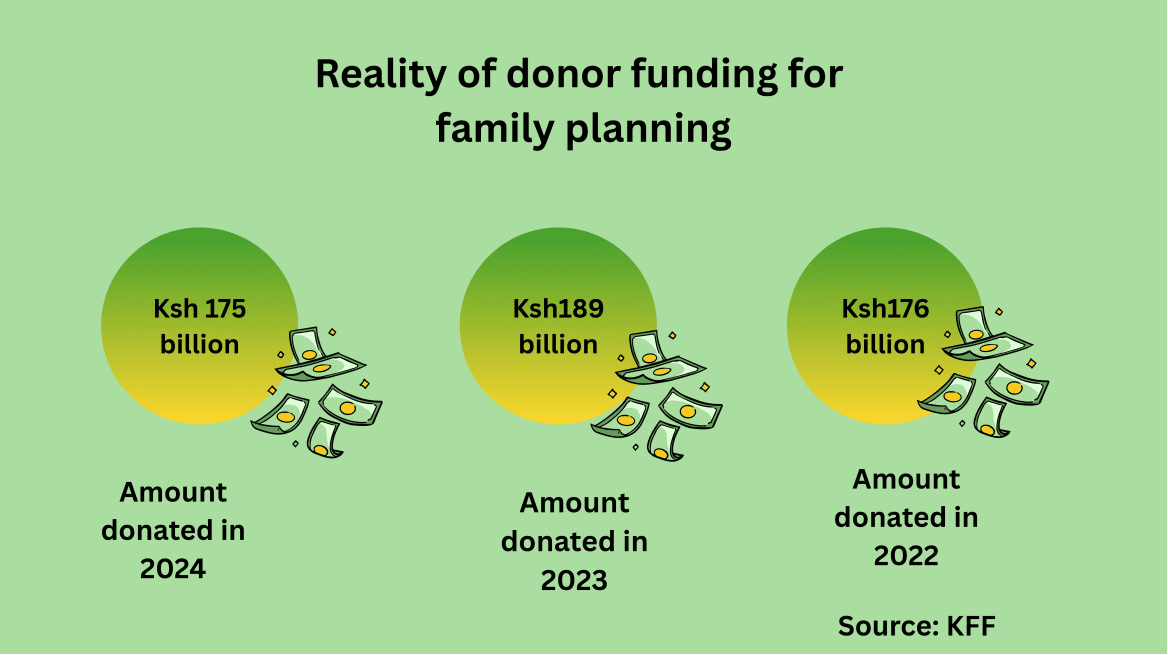
This response is unfolding at a moment of global donor retrenchment. A report by KFF, an independent source for health policy research, polling and news, shows that funding for family planning declined by 8%, from Ksh 189 billion in 2023 to Ksh 175 billion in 2024, well below the 2019 peak of Ksh 203 billion.
Within this shrinking fiscal space, Youth Voices and Action Initiative (YVAI) has linked grassroots problem-solving to county budgets, national obligations, and African Union commitments—turning local innovation into a political claim for sustained public action.
An app, a brigade and a bargain with power
YVAI’s response was both practical and political. The organisation adopted the Hesperian Health Guide app, a Kiswahili, read‑aloud, low‑bandwidth tool that explains contraceptive options, maps which clinics have stock, and preserves user privacy. The app is paired with a trained network of Community Health Promoters (CHPs) who verify stock‑outs, report patterns, and help women find available services.
The technology does three things at once: it returns information power to women, it produces verifiable data on supply gaps, and it builds an evidence base for county procurement. “Technology helps women find where commodities exist,” Leila says. “But we do not stop there, we take that data to county officials and demand budgets and timetables.”
YVAI shares aggregated app data with Reproductive Maternal Newborn Child and Adolescent Health (RMNCAH) coordinators and uses it in public participation sessions to show where procurement must be tightened.
As a result, the county, Leila says, has piloted a similar digital reporting approach to track family‑planning commodities, an operational step toward linking civic data to county procurement.
According to Kenneth Miriti, Kilifi RMNCAH coordinator, the county has piloted a similar app to track family‑planning supplies as part of efforts to build resilient health systems.

Apart from the App, Leila has been instrumental in pushing for healthcare reforms at the county level. In 2021, she led the grassroots task force that helped design Kilifi’s reproductive‑health strategy.
She was also part of the coalition drafting the Kilifi RMNCAH Act 2024 — a county law assented by the governor that sets standards for quality, affordable and respectful care across the life course. The Act establishes a legal framework for county obligations on maternal, newborn, child and adolescent health and creates a stronger basis for budgeting and accountability.
Her advocacy is procedural and pointed and this is attested by the fact that YVAI participated in County Integrated Development Plan (CIDP) public participation forums and submitted memoranda calling for ring‑fenced family‑planning lines, CHP stipends to sustain referrals, and adolescent‑friendly services including childcare for young mothers in training programs.
She routinely brings app‑generated stock‑out reports to RMNCAH coordination meetings, framing data as an administrative demand: fix procurement, not just patch distribution.
“We act as a temporary bridge, a catalyst to help public systems function,” Leila says. “But our goal is to push the county to own the solution, budgets, procurement timetables, accountability.”
Rights, law and continental leverage
Leila frames her demands in legal and continental terms. Kenya’s Constitution guarantees reproductive health under Article 43 (1a), while devolution assigns counties responsibility for delivering many health services. The Digital Health Act 2023 further opens pathways for integrating tools like Hesperian into public health systems.
At the continental level, African Union frameworks such as Agenda 2063 and the Gender Equality and Women’s Empowerment (GEWE) Strategy commit member states to advance women’s health and eliminate barriers to reproductive rights.
These frameworks carry political weight. Leila uses them as leverage, arguing that when counties fail to budget for contraceptives or integrate digital reporting, it is not simply a local management lapse but a breach of national and continental obligations.
“Agenda 2063 and the AU gender strategy give us a lever,” she says. “They make it possible to press county actors on obligations that go beyond politics.”
The stakes are clear. Kenya increased contraceptive use from 32% in 2003 to 57% in 2022, while unmet need declined from 27% to 14%. These gains are now at risk as funding declines and supply systems become more unstable.
YVAI measures two outcomes: access and agency. Access asks whether commodities are available when and where they are needed. Agency considers whether adolescents understand their bodies and can make informed choices.
The app reduces wasted trips and generates real-time evidence on stock-outs, while adolescent “power” circles build menstrual literacy, expand knowledge of contraceptive options, and strengthen confidence to seek services. Trained community health volunteers improve referral completion and reduce loss to follow-up.
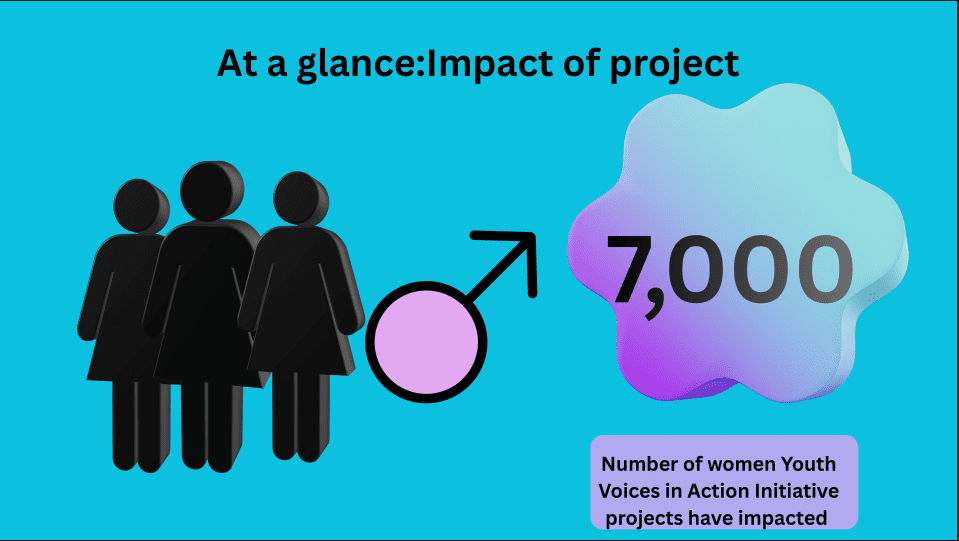
So far, YVAI has reached over 7,000 adolescent girls and young women, combining digital tools, community networks, and advocacy to address both supply and demand gaps in family planning.
Leila is now pushing to institutionalize these gains. She advocates for integrating YVAI’s indicators into the county RMNCAH dashboard so that community-generated data becomes part of formal monitoring systems. “If our indicators are in the dashboard, the county cannot say it didn’t know,” she says.
Budget battles and the advocacy gap
Budget politics determine whether innovation scales. Leila presses for explicit, ring-fenced allocations for family planning within the CIDP and annual budgets—not vague percentages, but line items that can withstand mid-year reallocations. She also calls for Community Health Promoters’ stipends to be included in recurrent budgets, so referral systems are not dependent on donor funding.
Local officials confirm the challenge. Kenneth Miriti, the county RMNCAH coordinator, acknowledges that while United Nations Population Fund supplies commodities, gaps persist due to national procurement bottlenecks and shifting donor priorities.
He welcomes civic data that improve forecasting: “If we can see stock-out patterns early, we can adjust procurements and request funds through projects like the Building Resilient and Responsive Health Systems (BREHS).”
However, he cautions that county cash flow constraints and national procurement cycles continue to limit responsiveness.
The scale of the funding gap remains significant. Even with UNFPA allocating Ksh 387 billion (US$3 million) for contraceptives in 2025, combined resources cover only 17% of national need, leaving counties to manage persistent shortages.
In response, YVAI is piloting livelihood and digital literacy programmes to reduce dependency and ensure women can effectively use and benefit from the app. Yet Leila is clear that these interventions are not a substitute for functioning public health systems.
She advocates for structural reforms: integrating app-generated data into the county health information system, incorporating CHP stipends into recurrent budgets, and ring-fencing procurement funds. Only then, she argues, can innovation serve as a complement to, rather than a replacement for, public service delivery.
Her asks are precise: “We need to adopt a ring‑fenced family‑planning commodities line in the CIDP and annual budgets.” She also underscores the need to integrate Hesperian‑generated stock‑out reporting into county procurement forecasting and the RMNCAH dashboard.
Leila further says there is need to fund CHP stipends to sustain referral networks and invest in adolescent‑friendly services and childcare support to ensure continuity for young mothers seeking training.
Kilifi’s stock‑outs are a symptom of a broader implementation gap. Kenya reports to continental bodies on health and gender commitments; subnational performance must match those reports.
When counties fail to ring‑fence funding or operationalise national procurement plans, Kenya’s ability to demonstrate real progress to the AU and other partners is compromised. Leila’s approach, which produces subnational evidence, pressing for line items, and citing constitutional and AU obligations makes local accountability traceable and auditable.
Stories from the field
Leila and her organization, runs a programme called “Building Adolescent Girls Power”, targeting girls between 10 to 19 years. One of the programme participants, Mekatilili, 17-year-old girl attests that since being incorporated into the programme, her mindset has shifted. She describes the “power” circle as transformative: “Nimejifunza mengi kutokana na hii programu kama kujua mzunguko wangu wa hedhi, njia za kujikinga na pia njia mbali mbali za kuzuia kupata mimba” (I have learnt a lot, how to track my menstrual cycle, ways to protect myself and the available contraceptive options) she says. From the training, she now mentors peers.

CHPs report fewer wasted journeys by women searching for supplies; clinic logs show faster referrals from YVAI‑linked CHVs.
The RMNCAH Act, the app pilot and documented public participation are tangible outputs that shift the debate from charity to duty. But Leila knows numbers matter. She is pushing to have the app’s aggregated stock‑out data published and to see CHP stipends and commodity lines appear in the next CIDP budget book.
Despite the efforts, Leila faced some backlash. Most of the community elders initially resisted family‑planning messaging; she recalls village meetings where she and her team were accused of “promoting immorality.” As a result of her persistent engagement, she turned critics into allies: one of the village elders now recommends the program publicly.
Yet political resistance can be stronger in budget rooms. Convincing MCAs to ring‑fence recurrent funds requires sustained civic pressure and clear, auditable evidence that budgets will reduce maternal harms.
Leila’s work crystallises a critical question: can grassroots innovation compel fiscal change? She has the tools that include data, legal framing, public participation and the constituency. The next test is whether county assemblies convert memoranda and app evidence into line items and whether procurement timetables shift from emergency buys to predictable forecasting.
A wider lesson for AU commitments
YVAI’s campaign illustrates a wider AU challenge: continental commitments require subnational follow‑through. Agenda 2063 and the AU Gender Strategy call for universal access to reproductive health. Achieving those goals demands counties that can plan, budget and procure.
By converting app data into political pressure, Leila creates a replicable model: civic data generation, public participation, legal framing and budget advocacy, a method that other counties across Africa could adopt to translate AU ambitions into local realities.
YVAI’s model demonstrates how grassroots innovation can close information gaps, mobilise demand, and generate auditable evidence. But Leila’s strategy is clear: technology and outreach are only leverage if county governments respond with budgets, procurement discipline, and legal recognition.
Without sustained domestic financing, Kenya risks reversing hard-won gains in reproductive health as global funding continues to decline and local systems remain under-resourced.
By taking app data, community testimony, and adolescent outcomes into county forums, Leila turns innovation into a political claim: adopt the budgets, integrate the data, and meet national and African Union obligations—or explain why you will not.

Leave a Reply