
Making psychological therapy affordable to children in Kenya
In Kenya, thousands of children struggle with mental health challenges, yet access to care remains limited by cost, stigma, and systemic gaps. As national policies lag behind growing need, grassroots initiatives are stepping in to bridge the divide by offering support where formal systems continue to fall short.
“I created a safe space for children—a space I always wanted to have as a child.”
More than 12 years ago, Mary Akinyi lost her mother. As a child, she struggled to understand the cause of her mother’s death, carrying unanswered questions into adolescence.
“My mother was constantly crying, but she would wipe her tears and tell me I wouldn’t understand,” Akinyi recalls. At the time, her mother had been treated for headaches and a short illness. It was only years later, after studying psychology, that Akinyi came to understand that her mother had been living with severe depression, undiagnosed and untreated.
What she did not yet realise was that her mother’s experience reflected a broader gap in Kenya’s health system, where mental health conditions often go undiagnosed, underfunded, and misunderstood.
Akinyi remembers her mother becoming increasingly withdrawn—speaking to herself, expressing thoughts about death, and gradually losing the ability to care for her family. What appeared to be physical illness was, in reality, prolonged psychological distress that eventually took a toll on her body.
“Back then, stress was not considered a disease, so she never went to the hospital,” she says. Healthcare affordability remains a major barrier for many low-income families in Kenya, particularly when it comes to mental health services. Limited awareness, cultural stigma, and financial constraints continue to restrict access.
The hidden crisis
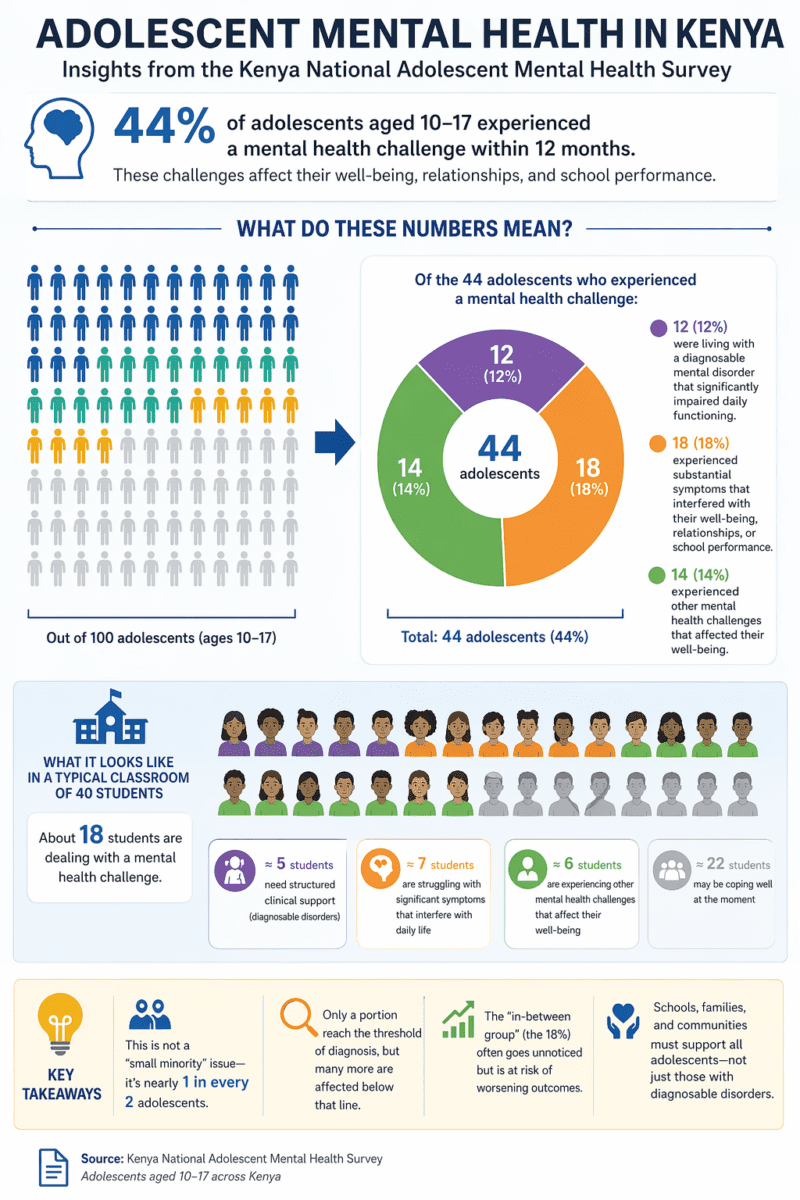
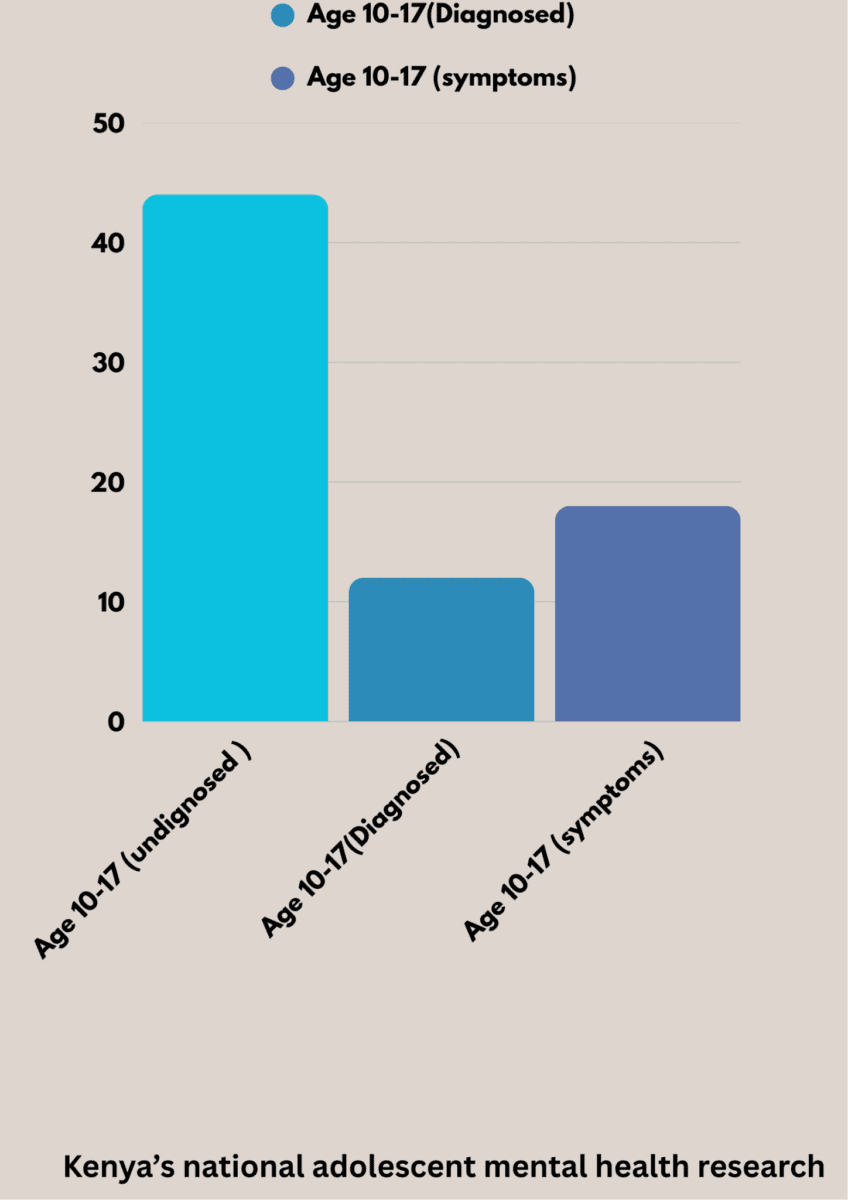
According to the Kenya National Adolescent Mental Health Survey, 44% of adolescents aged 10 to 17 experienced a mental health challenge within 12 months, affecting their well-being, relationships, and school performance.
Of these, about 12% were living with a diagnosable mental disorder that significantly impaired daily functioning, while a further 18% experienced substantial symptoms that interfered with their lives. Despite this, access to affordable, child-focused mental health services remains limited, especially for low-income households.
At 14, Akinyi herself began experiencing anxiety and depression as she processed grief without adequate support. After being sent to live with her grandmother, her struggles deepened, pushing her into a survival mode that would later shape her life’s work.
Years later, she enrolled in a psychology course at Moi University, driven by a desire to help children and parents navigate the kinds of challenges she had faced.
While all children are vulnerable to psychological challenges, experts warn that those in single-parent households often face greater risk due to emotional strain, financial pressure, and limited parental support. This was the case for Deborah (not her real name), who struggled to understand the changes in her daughter’s behaviour.
Her 14-year-old daughter began spending long hours locked in her room—curtains drawn, windows shut—sitting in darkness, withdrawn and increasingly distant. Like many parents, Deborah initially dismissed it as a normal phase of adolescence.
Afraid of being perceived as a failed parent, she responded by correcting and disciplining her, hoping things would improve. Instead, the distance grew. “It disturbed me that my daughter had become rude, distant, and secretive. She used to be happy and respectful, but she had completely changed,” Deborah says.
Looking back, she traces the shift to a few years after the death of her husband. In trying to fill that gap, she threw herself into work. “I was trying so hard to provide, not realising that while I was physically present, I was emotionally absent,” she says.
As time passed, the situation worsened. Her daughter began showing signs of depression, experimenting with substances such as cannabis and alcohol, and withdrawing further from family life. Attempts at discipline, including physical punishment, only escalated the problem.
“It was only after speaking to a therapist that things began to change,” she says. After overcoming the stigma of seeking help, Deborah enrolled her daughter in therapy at Arukah. “During the counselling sessions, I began to understand something painful but important: my daughter didn’t just need provision, she needed presence. She was carrying grief, confusion, and loneliness that I had not seen because I was focused on surviving and providing.”
Session by session, both mother and daughter began to heal, gradually rebuilding their relationship. “I thought being a good parent meant providing. Now I understand that being emotionally present in your child’s life is just as important,” she says.
Unaffordable care
Yet for many families, access to such support remains out of reach. Pamela Nasimiyu, a single mother of four, faces a similar struggle. She recalls receiving a call from her mother-in-law warning that her 16-year-old daughter was threatening to run away and live on the streets.
Her children had spent years moving between relatives as she worked in Nairobi to support them. She had also left her marriage after enduring prolonged conflict and abuse—experiences that left both her and her children grappling with fear and anxiety.
Findings from a study titled The Prevalence of Psychological Problems of Students from Single-Parent Families suggest that many children raised in single-parent households struggle with low self-esteem and heightened levels of anger. Many also experience symptoms of depression and anxiety, which interfere with concentration, motivation, and overall school performance.
For Pamela, this reality is deeply personal. The separation from her husband, though necessary for safety, added another layer of emotional strain to her family. Her eldest son, once full of ambition, now feels stuck and overwhelmed, unsure of how to move forward. Cultural expectations have further complicated his situation, as inheritance norms limit his ability to claim land after his mother left the marriage.
Her youngest son, in Grade 7, has grown increasingly withdrawn, barely speaking—a silence that reflects unspoken fear and emotional distress. Her third-born, now in Form Three, has also retreated into himself, using isolation as a coping mechanism.
“I don’t know where to get help. What I earn is too little, and I have to balance between school fees and feeding,” she says. For Pamela, therapy remains both inaccessible and unaffordable. Like many parents in similar situations, she can only hope that time will ease her children’s struggles.
A child-centred solution
For many families, the lack of accessible mental health support leaves few options, forcing them to navigate complex challenges alone. It is this gap that drove Akinyi to act. In late 2024, she founded Arukah Safe Haven to provide free therapy to underserved children and parents. The initiative works through schools, churches, and community support groups, with dedicated programmes for vulnerable children, including those living with sickle cell disease.
Her approach is simple but deliberate: to offer accessible, child-focused mental health support for young people aged 10 to 18 facing anxiety, depression, and other psychological challenges. Akinyi’s work is grounded in Kenya’s legal framework, which guarantees the right to health and upholds principles of equality and non-discrimination—rights that often fail to translate into practical support for children.
She was particularly drawn to the experiences of children from single-parent households—children like herself. Many parents described their children as “stubborn” or “difficult,” while the children themselves felt unseen and unheard. For Akinyi, these stories echoed her own.
She began as a volunteer, offering counselling to both children and parents. Over time, her work evolved into structured programmes delivered in schools, churches, and specialised support groups. Yet her work unfolds against a much larger national challenge.
Kenya is facing a growing mental health crisis. An estimated 5 to 10 million people—roughly 10 to 20% of the population—are living with conditions such as depression, anxiety, substance use disorders, bipolar disorder, and schizophrenia.
Despite the scale of the challenge, mental health care receives less than 0.01% of Kenya’s national health budget—a fraction of the 5% recommended by the World Health Organization for low-income countries. This underinvestment reflects broader prioritisation gaps within the health system, where mental health remains one of the least funded areas despite rising demand.
At a broader level, initiatives like Arukah Safe Haven align with continental frameworks such as Agenda 2063 and the African Union’s Gender Equality and Women’s Empowerment Strategy, both of which emphasise youth well-being, inclusive education, and equitable access to services. However, the gap between policy commitments and implementation remains significant.
Multiple factors continue to drive the crisis. Poverty, trauma, and social and economic hardship—alongside the growing influence of digital environments—are intensifying mental health challenges, trapping many in a cycle where poor mental health and economic vulnerability reinforce each other.
Stigma further compounds the problem, discouraging individuals from seeking help and perpetuating harmful attitudes toward those living with mental illness.
Environment impact
The Kenya National Adolescent Mental Health Survey identifies anxiety disorders as the most common condition among young people, affecting more than a quarter of adolescents. Depression is also a major concern, particularly among older teens. Trauma-related symptoms and behavioural difficulties are especially prevalent among those who have experienced loss, violence, or other forms of adversity.
Experts emphasise that beyond individual experiences, a child’s environment—at home, in school, and within the community—plays a critical role in shaping mental health outcomes.
Loice Okello, a counselling psychologist, underscores the importance of the home environment. “At the core, children need their basic needs met, but beyond that, they need to feel loved, cared for, and appreciated,” she says.
Children who grow up in supportive and nurturing environments are more likely to develop self-confidence and emotional resilience. In contrast, exposure to physical violence, emotional abuse, or harsh communication can leave lasting psychological harm.
Okello notes that unresolved emotional pain can lead to unhealthy coping mechanisms, including substance use and social withdrawal. “When children are pushed to focus only on achievement and image, they may begin to believe that success justifies any means,” she explains. “This mindset can later contribute to broader social challenges, including corruption.”
At the same time, she emphasises the need for balance. “While love and affirmation are essential, families must also teach discipline in a healthy and structured way,” she says. “Children who grow up in abusive environments may normalise that behaviour and replicate it in their own relationships.”
Without adequate guidance and support, children may struggle to navigate social environments such as school or places of worship. This can lead to rejection, bullying—both offline and online—and persistent criticism, all of which can trigger anger, self-stigma, and hopelessness. “When emotional distress is prolonged and unaddressed, it can escalate into suicidal thoughts or self-harming behaviours,” Okello warns.

Coordinated response
Despite growing awareness, systemic challenges continue to limit the effectiveness of mental health interventions in Kenya. Chebet Birir, a mental health advocate, journalist, and founder of Restored Minds Akili Care Kenya, argues that addressing these challenges requires a coordinated, multi-level approach.
She calls on the government to prioritise mental health by increasing funding, fully implementing existing policies, and ensuring that all healthcare facilities provide consistent counselling and psychiatric services.
She also emphasises the need to integrate mental health education into school curricula and make counselling services accessible to students. In addition, she recommends the development of national helplines and digital platforms to expand access to support. “Working with organisations, schools, community centres, and employers allows for pooling resources and expanding reach,” she says.
Birir further highlights the importance of culturally responsive care, where therapists adapt their approaches to reflect the social and cultural realities of their clients. She also points to the growing role of digital tools in delivering accessible mental health education and counselling services.
Within schools, she stresses the importance of involving parents in the therapeutic process, while ensuring that privacy and scheduling are handled carefully to avoid stigma or disruption to learning. For institutions with limited resources, she recommends shared or visiting therapist models as a practical alternative.
She also underscores the role of employers in advancing mental health awareness, suggesting that workplace wellness programmes can support both employees and broader community initiatives.
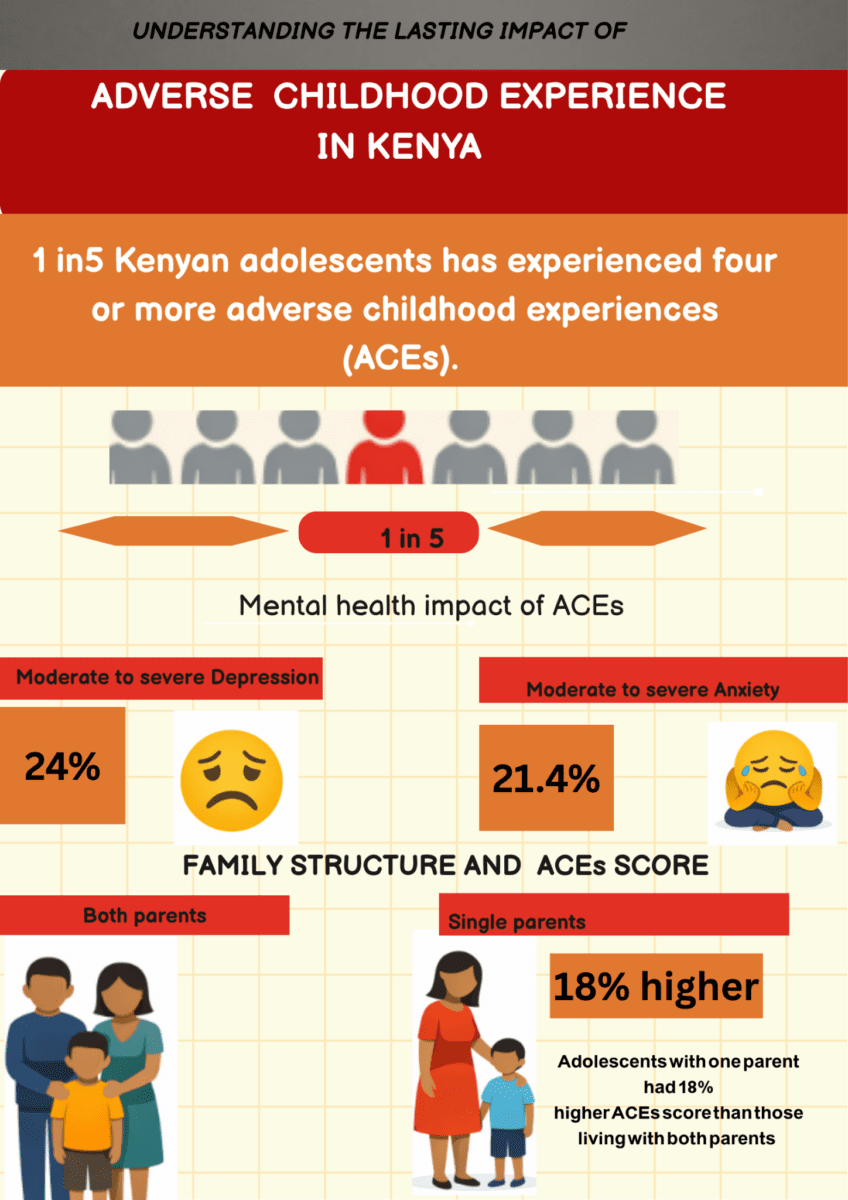
According to Birir, sustainable progress will depend on collaboration, innovation, and sustained investment. These challenges are reflected in emerging evidence. A study titled Understanding the Lasting Effects of Adverse Childhood Experiences found that one in five Kenyan adolescents has experienced four or more adverse childhood experiences (ACEs).
Young people with higher ACE scores were significantly more likely to experience mental distress—24% reported moderate to severe depression, while 21.4% experienced moderate to severe anxiety. Adolescents from single-parent households recorded ACE scores 18% higher than those living with both parents, underscoring the compounded risks faced by vulnerable groups.
Okello points to early warning signs that are often overlooked. Sudden behavioural changes—such as loss of interest in activities, disrupted sleep, neglect of hygiene, emotional numbness, and frequent physical complaints like stomach aches or migraines—can all signal underlying stress.
She also highlights “role reversal,” where children are forced to take on adult responsibilities due to illness, death, or family conflict. “The child must be supported and empowered, while the parent must also receive therapy,” she explains.
Policy gaps
“What we lack are the structures, trained personnel, resources, and motivation to put existing policies into action. Once the government commits the necessary support, we may not need to reinvent the wheel.”
These challenges persist despite the presence of national frameworks intended to guide mental health services. The Kenya Mental Health Policy 2015–2030 recognises children and adolescents as a vulnerable group and calls for their inclusion in planning and service delivery.
It also promotes integrating mental health care across sectors such as education, healthcare, and community services to enable early identification and intervention.
However, while the policy acknowledges children’s needs, it provides limited child-specific implementation pathways, instead embedding them within broader system reforms. This gap continues to constrain practical impact.
For Akinyi, bridging the gap between affordability and stigma requires collaboration. “While free therapy is important, it is not sustainable on its own. We need stronger structures and partnerships to scale,” she says.
The scale of unmet need is reflected in recent research. A study published in Social Psychiatry and Psychiatric Epidemiology found that 37.7% of upper primary school children in Kenya met the criteria for at least one mental health disorder.
The most common issues included physical complaints linked to emotional distress (29.6%), followed by affective disorders (14.1%) and conduct disorders (12.5%). About 18.2% of the children experienced multiple mental health conditions.
These findings underscore how widespread mental health challenges are among school-aged children. Akinyi identifies underfunding as the single greatest barrier to care. She calls for increased investment in community-based counselling and the integration of mental health services into primary healthcare systems.
“When funding is this low, services remain out of reach for those who need them most,” she says. “We need sustained investment, not short-term projects.”
For Deborah, therapy has been life-changing, but access remains limited. “I was lucky to find support,” she says. “Many others are still struggling quietly because they cannot afford care or do not know where to turn. With more funding, more lives could be saved.”

Leave a Reply